- All You Need to Know
The stiff hip
The stiff hip asks if you can pull your knee to your chest?
There are two opposing conditions in the hip joint. This one causes too much coverage of the head of the femur; the feature of the other, dysplasia, is not enough as the socket is too shallow.
This is thought to be a hereditary condition whereas hip dysplasia is caused by the foetus not lying in the Lotus position in the uterus. It's the pressure of the ball that forms and moulds the acetabulum.
Too deep a socket doesn't cause much pain initially except when pulling the knee to the chest and opposite shoulder. The range of motion of the hip is grossly reduced with a hard end feel. In fact it feels clinically like the arthritic hip of an older person, but starts in the teenager.
Ever scratched your head because a young patient has what appears to be arthritis? It was only around 1990 that this was recognised as a syndrome. But it does progress unerringly to a full blown degenerative hip if not carefully managed.
- Home >
- Pubic bone pain >
- The stiff hip

Femoro Acetabular Impingement Syndrome comes in two forms, which usually coexist.
The first, pincer, is a deformity of the acetabulum. The second, cam, is a growth on the neck of the femur.
They limit movement of the hip, with different ranges of motion affected depending on the exact nature of the deformity. Often it's flexion and internal rotation, but each case is different.
Repeated forcible striking of the deformity against the labrum can and does damage the latter causing pain in the groin, often spreading down the thigh towards the knee.
This is an incurable condition; orthopaedic surgeons like to grind off the offending growths but it's not a simple procedure; the hip has to be partially dislocated. And it's likely to regrow.
FAIS has only been recognised for a relatively short period so no long term studies, either chiropractic or surgical, exist.
Notice the CAM deformities bilaterally, marked on your reading left, and the progressive arthritis, particular on the right.

This 55 year old man has had stiffness in both hips for many years. Three years ago pain began in the groins. Now he can barely get his socks on. He can't walk 9 holes on the golf course; he has to use the wagon.
Within three weeks of Chiropractic care, the range of motion has dramatically increased, he can get his socks on, though there is no decrease in the pain yet. He has twice walked 9 holes without painkillers. Still, it's not easy yet.
In the xray above a CAM deformity is clearly seen. Below, closer inspection shows that he has in fact mixed CAM-Pincer deformity in this, his right hip; in fact in both. Moderate degenerative change is seen. An orthopaedic surgeon expects a bilateral hip replacement within two years.
We'll see ...
Oh, Glucosamine Chondroitin sulphate for 12 months helped not an iota ...

- More detail about Femoro Acetabular Impingement syndrome ...
- Femoro Acetabular Impingement Syndrome research[1] reports that on average it takes over three years to make the diagnosis, and on average they had been examined by four doctors. Groin pain was the most common complaint. 13 percent had had unsuccessful surgery at another site, thinking it was referred pain.
Conversely, DEVELOPMENTAL HIP DYSPLASIA (DDH)

Conversely, Congenital, or Developmental Hip Dysplasia exhibits TOO LITTLE coverage of the ball by the socket. This woman (42) too has bilateral groin pain, but with an increased range of motion.
Notice the steeply sloping roof of the acetabulum, yet the ball is not markedly unroofed. A mild case of DDH so no degenerative change at this stage.
DDH too has a prediliction for hip arthritis, but for different reasons. The shallow socket means a smaller area of ball-socket contact to support the full weight of the body, thus greater pressure directly on the cartilage: increased wear and tear.
- DEVELOPMENTAL HIP DYSPLASIA ...
- DEVELOPMENTAL HIP DYSPLASIA Ortolani Galeazzi tests improve the possibility of early diagnosis.
Both these women, one with Femoro Acetabular Impingement Syndrome and the other with Hip Dysplasia are responding well to a chiropractic regimen, and have much less pain, though the range of motion in the FAIS case remains limited, though markedly improved.
What is well understood is that any process that reduces the movement in a joint leads inexorably to Immobilisation Arthritis. Joint cartilage is perfused by the inarticular fluids, bringing oxygen and nutrients, and removing waste products of metabolism. Reduction of this perfusion is now well known to be noxious for joint cartilage.
Paradoxically, an increased range of motion also leads to hip arthritis.
Two mechanisms
In both mechanisms of Femoro Acetabular Impingement Syndrome there is increased contact between the acetabular rim (the labrum) and the femoral head / neck juntion. In both there is restricted flexion and adduction of the flexed hip, but rotation restriction is quite different.
Clinically, the presentation is one of a "stiff, non-painful, non-arthritic" hip in the early stages, the patient usually not realising that something is amiss. They regard it as normal, and do not report it. It is only discovered by the astute Chiropractic physician who is being thorough in his/her examination.
"If you do not look for it, you probably will not find it."
- Barrie Lewis D.C.
If not detected, the stiffness associated with Femoro Acetabular Impingement Syndrome in the young patient progresses to pain, primarily in the groin, frequently radiating into the Adductor Magnus which becomes extremely tender on deep palpation. Often there is associated sacro-iliac joint pain. The chicken-egg question often arises. Subtle, early degenerative changes of the acetabular labrum may now be seen.
Repetitive shock in sport between the femoral neck and the anterior wall of the acetabulum eventually result in these degenerative changes and may even result in an avulsion of the antero-superior acetabular labrum with very sharp stabs of groin pain.
1. Femoral neck deformation (aka CAM)


In CAM there is an abnormality at the level of the anterior femoral head, or the head-neck junction, resulting in increased femoral neck/head - acetabular rim contact. Cartilaginous lesions form along either the postero-inferior or superior aspects of the acetabulum, causing stiffness and limiting the range of motion. A hard end-feel is characteristic.
There is limitation of flexion, often adduction, and characteristically limited INTERNAL ROTATION, with a hard end-feel (in the young person, continuing of course into degenerative old-age arthritis, indistinguishable from conventional Cox arthritis, if not recognised and appropriately treated).
In Figure 1 there is no sign of CAM. The patient has absolutely no limitaton of internal rotation, but Faber is extremely limited. But there are strong signs of ...
2. Acetabulum deformation (aka PINCER)
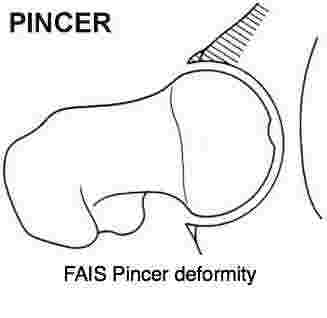
In Pincer-Femero Acetabular Impingement Syndrome - the acetabulum gives increased coverage of the femoral head - femoral neck juntion, limiting the full range of motion of the hip. In particular, EXTERNAL ROTATION of the flexed hip is characteristic, again with a hard end-feel.
Genetic influences
In a sibling study of 64 patients treated for primary impingement
deformities and osteoarthritis, a British group reporting in J Bone
Joint Surg Br found a 2.8 times greater risk if a sibling had a CAM
deformity, and 2.0 times for a Pincer deformity.
J Bone Joint Surgery Br 2010 Feb;92(2)
Fabere sign
In the Pincer form of Femoro Acetabular Impingement Syndrome, the Fabere sign is strongly positive:
F - Flexion
Ab - Abduction
ER - External Rotation
- Place the foot of the stiff hip on the opposite knee.
- The examiner places one hand on the opposite ASIS and the other hand on the knee of the affected leg.
- Pressing down on the knee of the affected leg immediately produces restriction, a hard end feel, and pain in the groin. The patient tends to roll the whole pelvis to reduce the pain in the groin as the examiner does the Faber test.(Pain in the SI-joint may also occur if there is a concomitent Sacro-Iliac syndrome)
- If the condition is bilateral, doing a double Fabere test immediately reveals that the patient cannot open (abduct) the thighs in the normal way.
E - Extension
A FAIS-Pincer sufferer would find it
quite impossible to sit in the lotus position. In the early stages it's
not painful, they simply cannot do it. Stiffness. In contrast the
patient with Developmental Hip Dysplasia is hypermobile, and would find
the lotus routine. In fact she can do it spectacularly with ease. She
can probably put her feet behind her ears too!

3. Mixed femoral neck AND acetabular deformation
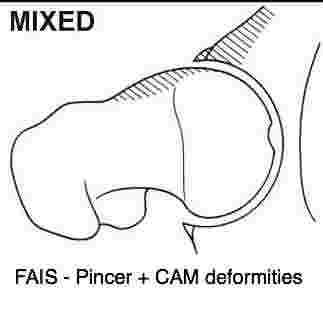
Nearly 90% of those suffering from Femoro Acetabular Impingement Syndrome have the mixed form, with both internal and external rotation limited. Only about 10% have either limited internal or external rotation.
Always with the characterisitic sign: BONE ON BONE, HARD END-FEEL. It's quite unexpected in the young person, and the arthritis associated with hard end-feel that we would expect to find simply is not seen on the x-ray.
Hence the paradox: A hard end-feel characteristic of arthritis, but no degenerative change; not yet. Unmanaged with good chiropractic, it will as surely as night turns to day, form a typical Cox joint in the future.
How common are these hip syndromes?
They are certainly not uncommon. This week I gave a lecture to 30 young adults on conditions that lead to hip arthritis. I was surprised that five of them had significant hip and groin issues. Four of them had hypermobile hips with pain in the groin suggestive of hip dysplasia.
One had very stiff hips with a positive anterior impingement test, but no pain. That is very suggestive of femoro acetabular impingement syndrome. None of them had x-rays so no diagnoses were forthcoming.
From a different perspective
Positive Impingement sign - ANTERIOR FAIS
- FAdIR
Flexion + Adduction + INTERNAL Rotation
With the patient lying supine, the examiner flexes the hip to 90*, adducts and then internally rotates. Restriction with a hard end feel, and pain in the groin is indicative of Femoro Acetabular Impingement Syndrome - CAM.
- FAdER
Flexion + Adduction + EXTERNAL Rotation
Now the examiner externally rotates the flexed and adducted hip. Pain in the groin and limitation of external rotation is indicative of Femoro Acetabular Impingement Syndrome - PINCER.
- Drehmann sign
Flexion + passive EXTERNAL rotation
Drehmann sign is positive with pain in the groin with Flexion and External rotation. Obviously this is very similar to FAdER restriction, and indicative of Pincer.
Positive Impingement sign - POSTERIOR FAIS
- ExER
With the patient lying prone, the examiner extends the hip, and EXTERNALLY ROTATES the hip (foot towards the midline).
Pain in the groin with a hard end feel is POSTERIOR Femoro Acetabular Impingement Syndrome.
Here are more thoughts on diagnosing the stiff hip.
From the chiropractic coalface
Mr S, a 42 year old man, consulted me some 12 months ago with extreme stiffness and pain in the left lower neck. X-rays revealed quite advanced degenerative changes in the cervical spine. Routine ROM testing elicited the chronic severe stiffness on left rotation.
On further investigation, in was immediately apparent that flexion, adduction and internal rotation of the left hip was also severely limited with an abrupt hard end-feel. X-rays revealed NO degenerative changes in the hip.
What I find interesting is that he belongs to a group of perhaps 1-2% in whom it almost impossible to get an audible release in the neck.
Clinically, with the protocol that I have developed for the hip, range of motion has improved dramatically (within a month), but the improvement in his neck has been much slower. After a year of treatment (2/w x 4w, 1/w x 3w, now 1/6w (15 in all) he has absolutely no restriction in the hip, and the neck has little pain, but the ROM is still restricted.
Postulated: The early diagnosis of Femero Acetabular Impingement Syndrome and appropriate treatment of the hip has resulted in a dramatic improvement in the hip, but the late diagnosis of the neck points to a far poorer prognosis. Understanding the mechanisms involved in Immobilisation Arthritis helps to explain the underlying disease process. More about IMMOBILISATION ARTHRITIS... Is there a connection between the stiffness in the neck and the hip? Is it coincidence perhaps. Certainly he has no psoriasis.
"THE LIFE SO SHORT, THE CRAFT SO LONG TO LEARN."
- HIPPOCRATES
Case File: Femoro Acetabular Impingement Syndrome
Here you can follow the progress of a new case. A middle aged man from the mixed CAM-Pincer Femoro Acetabular Impingement Syndrome CASE FILE with debilitating bilateral groin pain making walking very difficult. Golf only from a cart, with two anti-inflammatories to start the day. Read more from the Femoro Acetabular Impingement Syndrome CASE FILE
Mixed FAIS and DDH syndrome
Very occasionally, FAIS and DDH appears to co-exist in the same hip. It confuses all and sundry... MIXED FAIS DDH SYNDROME ...
From the literature
A group of orthopaedic surgeons reporting in Clin Orthop Relat Res. (2009) relate:
- Femoroacetabular impingement (FAI) is considered a cause of labrochondral disease and secondary osteoarthritis.
- Pain occurred predominantly in the groin (83%).
- The mean time from symptom onset to definitive diagnosis was 3.1 years.
- Patients were evaluated by an average 4.2 healthcare providers prior to diagnosis and inaccurate diagnoses were common.
- Thirteen percent had unsuccessful surgery at another anatomic site.
PAIN IN UPPER LEG
Pain in upper leg can making walking a misery, plague your patient's
sleep and test your diagnostic ability. Chiropractic can do miracles
though for what many may consider a "medical" problem.
PAIN IN UPPER LEG ...
Chiropractic and hip arthritis
Does chiropractic have a contribution to make in the prevention of hip arthritis? I'm utterly convinced we do.
Firstly in the early diagnosis of abnormal hip movement, though it's certainly only the observant and conscientious clinician will will discover these conditions in the patient who consults him for neck pain.
Early diagnosis of Femoro Acetabular Impingement Syndrome means getting the patient onto early range of motion exercises long before he or she even knows they have a problem. Prevention. Everyone gives it lip service, few take it seriously. Just this week a patient reported that a friend died during hip surgery; from the anaesthetic, apparently.
Secondly, chiropractors are routinely treating babies with Colic Chiropractic, and the examination should include the hips, listening for the characteristic 'thunk' of the subluxating hip. If not discovered early, and the pediatrician can miss it on a bad day, or in a mild case, they will never have a normal socket.
Thirdly, by advising their patients early that their hips simply won't go all fifteen rounds, to accept that marathon running, break dancing, ballet and gymnastics are not for them, is crucial.
And fourthly, I am personally getting great results in the treatment of early and moderate hip arthritis. Sometimes frustratingly not, but on average great progress with incrased ROM and less pain.
Chiropractic first!
Management of the sacroiliac joint is central to the success of treatment of the stiff hip; change of gait has a profound knock-on effect throughout the pelvis, and in fact the whole body.
Diagnosing the stiff hip early is central to successful treatment and preventing an early hip replacement.
Did you find this page useful? Then perhaps forward it to a suffering friend. Better still, Tweet or Face Book it.
MONTHLY NEWSLETTER. Signed up yet? It is free.
BACK ISSUES
Chiropractic Help Backissues ... our monthly newsletter, click here for all the old issues.
- Issue #53: No short cuts to better health / Simple balance and quad strengthening exercises
- Issue #52: Needs an adjustment / Everything must change
- Issue #51: Elective surgery in the elderly / Cooling and reheating starches
- Issue #50: Make time for breakfast / Scrambled eggs and parsley
- Issue #49: Consulting a locum / Green salad /Eggs Florentine
- Issue #48: Hips and the sacroiliac joints/ Bacon and eggs
- Issue #47: Life without medication/ Eight coloured foods
- Issue #46: Lower backs and ankles/ kaempferol and cancer prevention
- Issue #45: Tingling, weakness and malaise/ vitamin B1
- Issue #44: Applying general chiropractic principles to the hand / Omega-3
- Issue #43: Art and science of chiropractic / Kale
- Issue #42: Tum sleeping / Flaxseed
- Issue #41: Adult potty training / Beetroot constipation
- Issue #40: Ominous lumbar signs / Too much medication?
- Issue #39: Swapping chiropractors / Butter is back
- Issue #38: Making a correct diagnosis / Make your own pesto in five minutes.
- Issue #37: Have your wisdom teeth out in the chair
- Issue #06: Safety on the Stairs / Ginger
- Issue #05: Safety in the home / Red foods
- Issue #04: Whiplash and the Joints of Luschka / Parsley
- Issue #03: How to stop falling / Danger of a low fat diet
- Issue #01: Tingling in the arms and hands / Apples
(PS. If you find them irrelevant to your needs or an exercise in tedium, one click will UNsubscribe you.)
