- All You Need to Know
Spondylolysthesis
The term spondylolysthesis may be spelt with an i instead of a y.
What is a FACET?
This condition in the low back often leads to chronic lumbar pain and sometimes lumbar stenosis and leg pain. There are two causes:
- TYPE 1: A stress fracture between the facet joints.
- TYPE 2: Degenerative wear and tear of the facets, changing the shape and orientation of the facets.
Both types allow the vertebra to slide forwards on its nearest neighbour below.
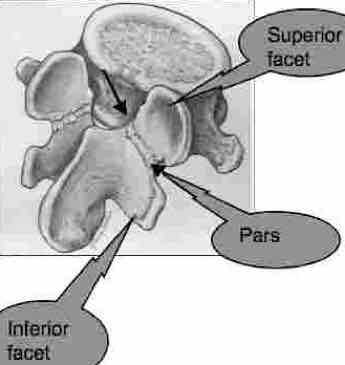
The spine fits together with an ingenious system of interlocking facets that click into the vertebra above and below. Each vertebra has four facets, two right and two left.
- Or two superior facets and
- two inferior facets.
Sometimes it's called an anterolisthesis.
Between the two facets lies the crucial weak area, the so called pars. Its full name is the pars interarticularis; a narrow isthmus of bone that links the two articular facets.
Notice the powerful, secure mechanism in the graphic below as the inferior facet of the vertebra of L4 locks neatly into the superior facet of L5. It's quite impossible for L4 to slide forwards on L5; unless there's a fracture in the pars of of the fifth lumbar vertebra.
A spondylolisthesis is diagnosed from an xray though the astute clinician may be able to palpate it. There is often a distinct abnormal relationship between the spinous processes as the body slides forwards and the posterior elements become more prominent posteriorally.
In order for the fracture through the pars to be seen a specific view, the oblique, must be taken. This enables us to see the scotty dog. And even then the fracture may not be clearly seen and a scan may be necessary, but only if you are not responding to treatment.
The fracture usually occurs in early childhood, though fast bowlers in cricket often get it. In that case it's really a stress fracture. But also any heavy fall onto the buttocks can fracture through the pars, as can a kick in the back in karate, for example.
Obviously, as with any fresh, new fracture, manipulation is contraindicated. Recently I have seen a healed bilateral pars fracture, but that's the exception. They don't usually heal because mostly they are diagnosed until months or years later.
A corset in my book is mandatory with a fresh pars fracture, and then it might heal.
Type I: Pars fracture Spondylolysthesis
SCOTTY DOG
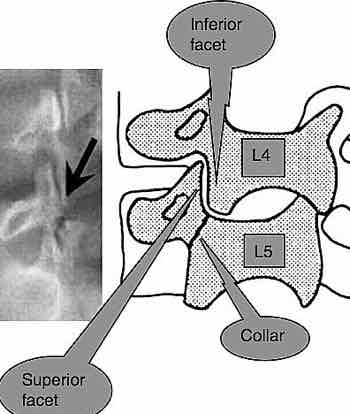
Can you spot the so-called "Scotty Dog"? If Scotty has a collar, then there is a defect. The defect itself is called a SPONDYLOLYSIS . It takes two 'Lysis', one on each side, to allow the vertebra to slide forward, the SPONDYLOLYSTHESIS.
Pars interarticularis
"inter" = between
"inter-articularis" = between the articulating facets.
Can you see the crack in the pars in the graphic above? Current opinion is that in childhood, when the pars is still made of cartilage, a heavy fall, or something ... it's almost never recalled, a fracture through BOTH pars interarticularises allows one vertebra to slide forward on that below.

Can you see how L5 has slipped forwards on the sacrum? Sometimes this puts the spinal cord under great stress as it must travel around two corners. Spinal stenosis may occurs - severe narrowing of the spinal canal causing lower back and leg pain ...
Type 2: Degenerative spondylolysthesis
If a lumbar joint has been fixated for a long period of time, immobilisation arthritis sets in at the facet joints. They change shape, become flattened and degenerate and allow the vertebra above to slide forwards, without a fracture in the pars. Nerve root impingement and chronic low back and leg pain are common.

CHIROPRACTIC HELP
In practice most spondylos due to fracture, or spondys as we call them, are usually stable. They cause discomfort and nagging pain periodically but no great dramas. They are seen in busy chiropractic clinics virtually every day of the week.
In my experience, all of thirty three years, the problem is often not at the spondylolysthesis, but at one of the adjoining joints. Either in one of the sacroiliac joints, or at the level above or below the spondylolisthesis. In this case, at the L4 L5 joint.
Spondylolysthesis is never cured, and must come under management by your chiropractor. I recommend an occasional, but regular, consultation. Daily exercises are essential, and an acceptance that playing silly buggers should have no place in the lifestyle of a person with a spondylo. Lifting pianos, heavy gardening and perhaps worst of all long periods of sitting do not belong in the life of person with a spondylolysthesis.
Now for a spondylolisthesis casefile.
As you will read in the casefile, degenerative spondys are often more difficult to manage than the first type, causing lower back and severe leg pain. Attention to detail by both doctor and patient
are vital. Ignore it, and you'll find yourself considering lower back
surgery, an unhappy prospect.
LOWER BACK SURGERY ...
FROM THE COAL FACE

Mr B, a 35 year old builder had Right low back pain for 10 years. In January 2008 it became severe, and radiated into the buttock, thigh, side of the lower leg and foot (pain, tingling and numb). He had to stay home for three months under physiotherapy. Lower back and leg pain is the norm...
Mr P consulted me in October 2008, still with severe pain in the buttock and right leg. Nonchalant walking, standing and sitting remained problematic.
His medical insurance was totally taken up with physiotherapy, but we agreed to a trial of 5 treatments. There was some progress with Chiropractic Help. I didn't see him again for three months during which time he progressively improved, coming in for another five treatments. Yesterday he told me he has no problem whatsoever.
Diagnosis:
- Sacro-iliac tests were strongly positive.
- Stable spondylolysthesis.
Treatment: 10 chiropractic treatments over a period of 8 months.
He is very faithful with his exercises and now comes every two months for an adjustment of his sacro-iliac joint.
In the x-ray above you can clearly see the crack through the pars.
Coalface 2

This is an altogether different kettle of fish. Mrs T, aged 62 first consulted me 6 months ago. She has had lower back pain most of her life.
Ten years ago she suddenly developed severe leg pain bilaterally, and was wrongly diagnosed with dystrophy in the lower legs by a neurologist. There are other causes of lower back and leg pain and clearly no xray was taken. She clearly has a serious spondylo with forward slippage, serious loss of disc height at L5 S1 and lumbar stenosis. Severe muscle weakness soon developed in both calves; at 52 she was unable to lift either heel from the ground. She was soon only able to walk with the aid of a walker. At the time, I would have recommended decompression surgery, not something I readily suggest, but it clearly should have been done; but it wasn't even considered.
Walking remained very difficult. Four years ago, because of the weakness in her lower legs, she had nasty fall resulting in the severe herniation at L2 L3. Pure misery over and above her other pain, with severe pain down the side of the right leg.
Notice the modic effect, deep bone pain caused by fluid that has seeped into the bone.
I won't pretend there have been miraculous changes. She still uses the walker, and the strength in her calves will never return. But the pain in her back is much reduced, she has almost no pain down the side of the leg, and she can sit without pain and is not woken in the wee small hours of the night. She comes every six weeks now for control as we call it in Holland. We're both very pleased obviously.
Update; one year later she is still doing very well. The strength will never return to her calf, so she uses a walker. It's really medical neglect though I'm unsure chiropractic could have done any better.
My point? This is a case where surgery was indicated ten years ago. It's too late now as the damage to the nerves to the lower legs is permanent.
Once your back pain has lasted more than six months, the
definition of chronic, the chances that your back pain will never
entirely go away increases. Living with back pain becomes
increasingly a reality. Learning to help yourself is always important.
That means more exercises.
Upper Thigh pain
Upper thigh pain may be a radiation from the upper lumbar spine as Maigne's syndrome, or a slipped disc affecting the femoral nerve, or it may be a hip condition, and frankly a host of medical conditions such as a prolapsed uterus. Careful evaluation is paramount.
OPEN ANDRE AGASSI
What a fascinating book! "OPEN" by Andre Agassi is un-put-down-able.
Read about how he survived spondylolisthesis to become the greatest
tennis player ever.
Lower back surgery
Surgery is not usually necessary for Spondylolysthesis but sometimes
there is severe loss of disc space leading to spinal stenosis and a foot
drop. Good surgery is an artform, bad surgery... a horror.
LOWER BACK SURGERY ...

Useful links
- The world needs hard working, honest and conscientious doctors: EDUCATION CHIROPRACTIC ...
- Go from "SPONDY" to LOWER BACK AND LEG PAIN ...
- Lumbar facet syndrome ...
- Sacroiliac joint treatment ...
- Delicious, fantastic mushrooms: NUTRITIONAL VALUE OF MUSHROOMS
- Go from SPONDYLOLYSTHESIS to CHIROPRACTIC HELP home page ...
Have A Question about your lower back?
I receive many questions about Chiropractic. It might be help with a spinal condition, but it might also be from a person who can't walk after a hip operation, or some such thing.
I will do that by answering your questions personally, but it will be converted to a Web Page so others can benefit from your questions. Omit your name if you like.
However, do understand that, in the main, I'm going to be directing you, should it be pertinent, to a Chiropractor in your neck of the woods. I'll respond to all reasonable inquiries, but please be specific, and give as much detail as you can.
Do understand that lower back pain is extremely complex, so I can only give general guidelines. There's no substitute for a careful thorough chiropractic examination.
What Other Visitors Have Said
Click below to see contributions from other visitors.
If you find my answer useful, please ask friends to grade it.
PAIN AND TINGLING IN FEET AND LEGS and toes from spondylolysthesis Not rated yet
Hi,
I have nerve pain/numbness in both legs and toes. I was diagnosed with spondylothesis of L3/L4 by spine specialist and put on nerve pain meds and …
"Gems, both funny and healthful, from the life and work of a chiropractor."
It won't be too many years before we read all books this way. Chopping down less trees, less room taken up by heavy bookcases, no more lugging heavy tomes about on holiday... you'll find the change to an eReader as easy as winking. Buy the cheapo...
Did you find this page useful? Then perhaps forward it to a suffering friend. Better still, Tweet or Face Book it.
MONTHLY NEWSLETTER. Signed up yet? It is free.
BACK ISSUES
Chiropractic Help Backissues ... our monthly newsletter, click here for all the old issues.
- Issue #53: No short cuts to better health / Simple balance and quad strengthening exercises
- Issue #52: Needs an adjustment / Everything must change
- Issue #51: Elective surgery in the elderly / Cooling and reheating starches
- Issue #50: Make time for breakfast / Scrambled eggs and parsley
- Issue #49: Consulting a locum / Green salad /Eggs Florentine
- Issue #48: Hips and the sacroiliac joints/ Bacon and eggs
- Issue #47: Life without medication/ Eight coloured foods
- Issue #46: Lower backs and ankles/ kaempferol and cancer prevention
- Issue #45: Tingling, weakness and malaise/ vitamin B1
- Issue #44: Applying general chiropractic principles to the hand / Omega-3
- Issue #43: Art and science of chiropractic / Kale
- Issue #42: Tum sleeping / Flaxseed
- Issue #41: Adult potty training / Beetroot constipation
- Issue #40: Ominous lumbar signs / Too much medication?
- Issue #39: Swapping chiropractors / Butter is back
- Issue #38: Making a correct diagnosis / Make your own pesto in five minutes.
- Issue #37: Have your wisdom teeth out in the chair
- Issue #06: Safety on the Stairs / Ginger
- Issue #05: Safety in the home / Red foods
- Issue #04: Whiplash and the Joints of Luschka / Parsley
- Issue #03: How to stop falling / Danger of a low fat diet
- Issue #01: Tingling in the arms and hands / Apples
(PS. If you find them irrelevant to your needs or an exercise in tedium, one click will UNsubscribe you.)
