- All You Need to Know
- Home
- Hip arthritis
- Hip Dysplasia Casefile
Hip dysplasia casefile
Hip dysplasia casefile yields important information about how undiagnosed disease progresses to full blown arthritis.
A 59 year old man presented at our clinic with sharp stabs of pain in the right groin that began approximately six years previously. An ache radiated down the front of the thigh to just below the knee.
He remarked that he had regular chronic mild lower back pain, but only rarely did it really trouble him.
The pain in the groin began gradually; it was intermittent but in the last six months it became much worse. He had difficulty reaching his shoe, walking caused sharp discomfort, and even cycling was restricted. Climbing stairs was a mission.
Remarkably, as most people have no idea how their mother's pregnancy went, he knew that he lay in the transverse position; she had told him.
Physiotherapy had brought a little temporary relief. Otherwise, nothing relieved the pain.
The ten questions in the questionaire at the bottom of this page will enable both you and your chiropractor to gauge
just how badly your hip pain is affecting your general life style. He rated his condition as an eight.
In this hip dysplasia casefile the patient stood with a distinct lop sided posture. A short left leg tilted his pelvis giving him a mild C shaped scoliosis.
The ranges of motion of the lumbar spine were as follows. Flexion was mildly pain in the low back. Backward bending and sideways to the left produced right LBP.
Hip Dysplasia CaseFile
Hip dysplasia casefile shows how undiagnosed and untreated DDH progressly inexorably on to arthritis.
Range of Motion of the right hip:
Flexion was severely limited to no more than 90* with a very hard "end-feel". That's typical of bone on bone. On flexing the hip to his chest, noteworthy was that he could only achieve it by simultaneously abducting the hip outwards. Likewise adduction, pulling it towards the opposite shoulder, was extremely restricted and caused sharp stabs of pain in the groin. Rotation, extension and abduction were relatively normal.
Motion palpation: The right sacroiliac joint was severely fixated (what I call a "feel of concrete" in the joint. It appeared "ankylosed".). Likewise there was a fixation of L5, the lowermost lumbar bone.
Orthopaedic testing:
Sacroiliac tests were negative. Yeoman's test produced mild L5 pain but nothing in the hip or SI joint. The Patrick Fabere test was normal surprisingly. Straight leg raise test of Lasegue only produced pain in the groin, ie. it was negative for a pinched sciatic nerve.
Hip arthritis
Hip arthritis is the natural consequence of every poorly managed hip dysplasia casefile; especially if there's a strong family association.
The radiologist's report reads as follows.
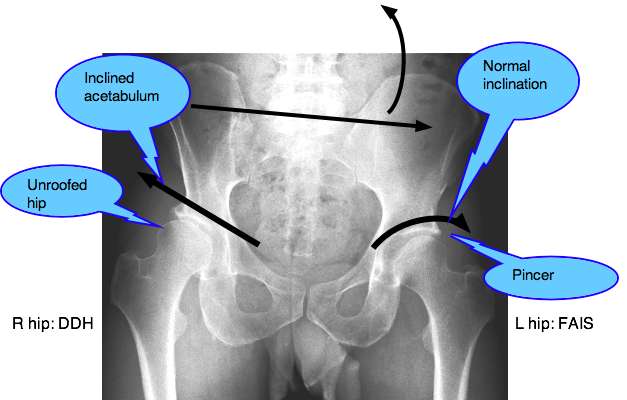
The right acetabulum lies more steeply inclined than the left hip. The cephalad portion of the hip joint is reduced in size, having worsened since the examination in 2005.
Bilaterally, there are degenerative changes occurring at the lateral margin of the roof of the socket. This has the appearance of a moderate Cox arthritis of the right hip associated with the mild case of dysplasia of the right acetabulum; normal sacroiliac joints.
Additional notes:
- Note the typical features on the right of developmental hip dysplasia; that's your reading left. The inclined,
sloping acetabulum compare with the normal socket in the left hip and the
unroofed portion of the ball.
- In the left hip there is concommitent femoro acetabular Impingement Syndrome Pincer.
- The tilted pelvis due to a short left leg.
- The mild curvature and degenerative changes of the lower lumbar spine.
DIAGNOSIS
Developmental Hip dysplasia casefile. DDH.
Chiropractic Help
Chiropractic help is unable to wave a magic wand over every hip dysplasia casefile. It takes a strong commitment on the part of both the doctor and the patient who avoid the natural progression of this disease to full blown hip arthritis.
I confess to becoming impatient with those not prepared to stick to the programme which might be summarised as:
- Disciplined daily exercises to strengthen the core pelvic muscles. it takes not more than two to three minutes, morning and evening. A regular swim would be beneficial.
- Eat those anti inflammatory foods that keep the anger in the hyaline cartilage to a minimum.
- Watch your weight, mostly simply by avoiding high GI foods like white rice and refined flour products used in most cookies and cakes.
- Come for chiropractic help as directed.
If you don't like pain and disability, and want to avoid a total hip replacement, then do it; those who will not hear, must feel, as the Dutch saying goes.
Just this week a relative died, two weeks after an otherwise successful total hip replacement; a fatty embolus from the femur lodged in the lungs.
CONSULT 1 : (17 June) HISTORY AND EXAMINATION
Subjective: Right groin pain.
Objective: Moderate to severe loss of flexion and adduction.
Assessemnt: Right hip dysplasia casefile.
Plan: Hip and pelvic exercises.
Sacroiliac Joint treatment
Sacroiliac joint treatment after careful examination may be a large part of the secret to a successful outcome of any hip dysplasia casefile.
CONSULT 2 : (26 June)
S: R groin pain.
O: No change
A: DDH, X-rays have arrived.
P: Report of Findings.
- Briefly go through the history. All correct? Yes.
- Review findings of the examination.
- View the X-rays together. Note features of DDH.
- Explain something of the philosophy of
chiropractic, particularly in this instance how fixated joints (his hip)
has led to arthritis as the hyaline cartilage in the joint is starved
of nutrients and oxygen, and waste products are not flushed away causing
" immobilisation arthritis ".
HYALINE CARTILAGE ...
- What form the treatment will take, and the frequency. The importance of the three phases of treatment:
- Treatment phase: 2/w x 3-5 weeks, depending on progress.
- Rehab phase: Less treatment, more emphasis on exercises, and maintenance of the condition by the patient.
- Maintenance phase: No one can cure the condition. Occasional (probably 6-8 weeks) treatment to sustain the expected improvement.
- Nutrition: to be discussed later.
First Chiropractic treatment of the sacroiliac joints, lumbar spine and hip joint.
CONSULT 3 : 1 July
S: Hip definitely feels looser. No "after pain" from the treatment.
O: No change in the objective findings of this hip dysplasia casefile.
A: Progress.
P: Add Mulligan belt mobilisation of the hip.
CONSULT 4 : 6 July
S: Increased pain in the low back.
O: Extension and increased flexion low back pain.
A: Low back in unstable phase after first few treatments: aggravations.
P: Change in treatment of L5. Right-side-down chiropractic adjustment of L5. Supine Thompson drop treatment of the right SIJ. Mulligan mobilisation of the right hip.
CONSULT 5 : 10 July
S: Much less back pain since last treatment. Groin pain still severe when walking. Range of motion of the hip increasing.
O: No lumbar flexion pain. Hip flexion still restricted to 90 degrees. Adduction improving.
A: First range of motion increases, then pain should decrease.
P: Nutrition. Discussed the need for nutritional support for the cartilage in the hip joint. Recommendations:
- Great increase in fatty fish in the diet to increase
Omega 3 essential fatty acids, and vitamin D, vital in good calcium
metabolism.
- 1000 mg Cod liver oil per day.
- Chicken bones extract for a delicious soup is useful in the management of Hip dysplasia casefiles.
CHICKEN BONES BOUILLON ...
- Freshly ground Flax seed with muesli every day.
CHIROPRACTIC HELP Obesity in the Chiropractic Clinic and the virtues of Omega 3 in Flax seed.
One big plus: Mr F's weight is perfect.
CONSULT 6 : 13 July
S: Improving. Minimal back pain, Walking improving.
O: Pelvis still obviously low on the left.
A: Time for a heel lift. 5mm lift in the left shoe immediately reduces extension pain in the low back.
P: As before.
CONSULT 7 : 20 July HIP DYSPLASIA CaseFile
S: Magic. 80% less pain in the groin. Can now walk without pain, first time in six years.
O: Hip flexion still limited to 90*. "Concrete feel" in right sacroiliac joint is gone. Normal movment of SIJ on motion palpation.
A: Hard end-feel in the hip is much improved.
P: Mr F can flex his hip another 20* after the treatment. Must continue with the exercises to maintain the increased range of motion. Next consult two weeks. Begin rehab phase, and begin treatment on the left hip FAIS.
CONSULT 8 : August 8.
S: Mr F is a different man. Walking is almost normal, certainly painfree, though he does have a slight limp on careful scrutiny.
O: For the first time hip flexion BEFORE the treatment now exceeds 90*. Adduction remains very limited. No abnormal sacroiliac findings.
A: He's doing better than expected. The interesting question is to what extent the Chiropractic adjustment of the sacro-iliac joint subluxation is what has restored his walking, and how much to do with the actual treatment of the hip itself.
P: Add further pelvic stabilisation exercises. Treatment as before. Next treatment in four weeks.
Note: I personally have gone into semi-retirement, and have left the care of Mr F to my colleague. No further updates to this casefile alas.
DISCUSSION of this Hip Dysplasia casefile
- Mr F has a mild case of Developmental hip dysplasia. Mild
enough to not have been picked up at birth by the paediatrician and mild
enough not to be noticed until he was in his early fifties.
- But bad enough to seriously change his lifestyle
in his mid fifties, cause severe groin pain, and bad enough if left
untreated to lead to a total hip replacement in his early sixties.
Though the improvement in only four weeks is most heartening, he may
still need major hip surgery.
- Inability to walk and cycle readily has meant Mr F
has become mildly disabled, and without treatment would become
seriously so within a short time.
- His doctor, in Mr F's forties, never examined his hip or, if he did, he never knew what Chiropractic could do for hip joints.
- We give lip service to "a stitch in time..." and
"prevention is better than a cure" but in practice Medicine seems to
place very little emphasis on prevention in the management of joint
conditions. Had this condition been detected 10-15 years ago, when the
first signs were surely evident to the discerning doctor, it would have
saved Mr F a lot of pain, and his medical insurance a possible total hip
replacement.
- In the USA a typical hip replacement in 2010
costs in the region of $40 000. Add to that the rehabilitation, several
months out of work, the risks of embolism and the anaesthetic... it's
high time primary care physicians were taught to examine the hip for
early restrictions of motion, and to refer them appropriately. Any thing
less comes close to negligence.
- Health is additive. Mr F has two causative factors: The well known increased incidence of hip dysplasia associated with transverse position in utero (and a breech birth). And he has a short leg. Leg length inequality research also conclusively indicates that the increase in the wear and tear on hips and knees associated with a short leg causes arthritis. A simple heel lift in his twenties... an equally simple set of exercises for his hip in his forties, and things would be very different today for Mr F.
Have A Great Story About This Topic?
Do you have a query or comment about upper leg pain or, for that matter, tingling in the legs and feet?
What Other Visitors Have Said
Click below to see contributions from other visitors to this page...
Subluxated hips and sacrum pain Not rated yet
Subluxated hips and sacrum pain
Hello dr Barrie!
I dont know if you remember me, we had a mail conversation about my hip problems earlier, I have ehlers …
- Home
- Hip arthritis
- Hip Dysplasia Casefile
Did you find this page useful? Then perhaps forward it to a suffering friend. Better still, Tweet or Face Book it.
MONTHLY NEWSLETTER. Signed up yet? It is free.
BACK ISSUES
Chiropractic Help Backissues ... our monthly newsletter, click here for all the old issues.
- Issue #53: No short cuts to better health / Simple balance and quad strengthening exercises
- Issue #52: Needs an adjustment / Everything must change
- Issue #51: Elective surgery in the elderly / Cooling and reheating starches
- Issue #50: Make time for breakfast / Scrambled eggs and parsley
- Issue #49: Consulting a locum / Green salad /Eggs Florentine
- Issue #48: Hips and the sacroiliac joints/ Bacon and eggs
- Issue #47: Life without medication/ Eight coloured foods
- Issue #46: Lower backs and ankles/ kaempferol and cancer prevention
- Issue #45: Tingling, weakness and malaise/ vitamin B1
- Issue #44: Applying general chiropractic principles to the hand / Omega-3
- Issue #43: Art and science of chiropractic / Kale
- Issue #42: Tum sleeping / Flaxseed
- Issue #41: Adult potty training / Beetroot constipation
- Issue #40: Ominous lumbar signs / Too much medication?
- Issue #39: Swapping chiropractors / Butter is back
- Issue #38: Making a correct diagnosis / Make your own pesto in five minutes.
- Issue #37: Have your wisdom teeth out in the chair
- Issue #06: Safety on the Stairs / Ginger
- Issue #05: Safety in the home / Red foods
- Issue #04: Whiplash and the Joints of Luschka / Parsley
- Issue #03: How to stop falling / Danger of a low fat diet
- Issue #01: Tingling in the arms and hands / Apples
(PS. If you find them irrelevant to your needs or an exercise in tedium, one click will UNsubscribe you.)
- Home
- Hip arthritis
- Hip Dysplasia Casefile
