| Back to Back Issues Page |
 |
|
CHIROPRACTIC HELP #51: Elective surgery in the elderly March 28, 2018 |
DearElective surgery in the elderlyElective surgery in the elderly is a difficult and controversial subject. The older person is vulnerable; almost without exception they are open to abuse by doctors, chiropractors and lawyers, for example, who see easy pickings.Could that arthritic hip or spinal stenotic neck be helped by surgery, or are the risks so great that it's not worth the chance that you may be left worse off than before? It's not an easy decision and I believe that family and friends should play their part in the decision making. After nearly forty years in practice, it hurts me how some doctors, and that includes my own profession, perhaps well meaning, can't see and properly evaluate these risks. What are they?
Anaesthetic risksMuch has been written about the dangers of an anaesthetic in the very young and the elderly; it needs to be seriously weighed. Many years ago I had a much loved elderly patient who went for elective surgery for an arthritic knee. As her husband confided in me afterwards, the operation really helped her knee, but after the procedure she had no idea where she was walking. Overnight, senile dementia set in from which she never recovered.An anaesthetic is a nerve toxin and, in sensitive individuals, the risk needs to be carefully weighed. Are you coping with that arthritic knee, or has the quality of life become so miserable that it outweighs the risks of dementia? I've recently sent just such a patient for a hip replacement; waking you at night is an important factor; anything that disturbs your sleep is significant. Or are you actually coping and, whilst it's not great, you really are managing? The subject has touched me personally. Many years ago I went in for minor surgery that in those days involved a general anaesthetic. I felt dreadful for several weeks, not from the surgery, but from the effect of the anaesthetic. It was only later that I realised that I lost quite a few marbles, losing the ability to remember people's names unless I saw them regularly; the damage is permanent. Many years later the anaethetist confided in me that she very nearly lost me; my blood pressure dropped so drastically that there had been very real risk of my demise. It happens but I was lucky to escape with only some damage to the memory centre. Nerve risksSpinal surgery is a risky business, but is sometimes obviously necessary and unavoidable, especially when there is ongoing severe pain in a limb or loss of muscle strength, known as paresis. Pressure on the spinal cord in the neck can be so great that it may cause a far distant weak ankle, for example.Sometimes that surgery may actually exacerbate that risk to the nerve and seriously increase the pain and weakness in the limb. Whilst I have no figures at hand, if you read the disturbing letters sent to me at Chiropractic Help, you'll realise it's certainly not uncommon.
Spinal stenosis is another serious ongoing problem in the older person. Because of loss of disc space and degenerative changes around the nerve root, frank pressure remains likely in certain individuals, depending on the shape of the spinal canal, and swelling of the yellow ligament in the canal. Elective surgery in the elderly should obviously weigh all the risks against the expected benefits.
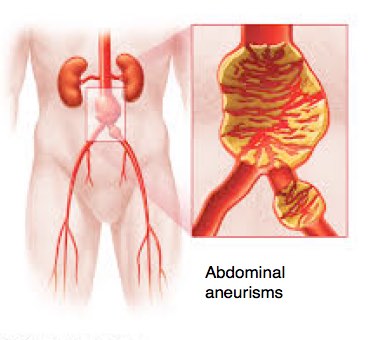
Surgical risksAre you coping with that problem, or is it so severe that because of loss of independence, or pain, or bowel function perhaps that you really have no option? It's not really elective surgery, because you have no alternative.I once had another favourite elderly patient who I sent for routine lower back x-rays; apart from his spine the radiograph revealed an aortic aneurism of about 45mm; after 40mm they quite often progress fairly quickly. I asked his doctor for an opinion, who referred him to a vascular surgeon.
Instead of a more conservative approach, weighing the risks of elective surgery in the elderly, he advised an immediate operation. Christiaan was a strong and active retiree. He played bowls twice a week, regularly with his wife took extended holidays in their caravan, and every year gave one of his children a much needed break from their citrus farm in the Cape; they would go and stay, taking care of the grandchildren and seeing to the every day business of the estate. He died two days after surgery. In retrospect, he should never have had that operation, instead going for a six monthly ultrasound exam to see if the aneurism was progressing. The downside risk of not having that elective surgery in the elderly was sudden death from a burst abdominal aneurism. These things need to be carefully weighed before elective surgery in the elderly; the opinions of friends and family, the family doctor and chiropractor should be solicited in my opinion. I had advised Christiaan not to go for that op; his wife never forgave me nevertheless, since I had discovered and initiated the chain of events that led to her husband's premature demise. Medication risksI have an elderly patient, ninety this year, whom I have treated for over thirty years. On x-ray his lower back looks dreadful at multiple levels but he has minimal pain, with occasional episodes of severe pain down the back of his left leg; twice in the last five years. Both times he responded well to gentle chiropractic adjustments of his spine and pelvis, and was painfree within a few weeks.He is an active, busy man, in good health; just recently he and his wife drove a thousand miles to Cape Town for the wedding of a grandchild; and back after a short holiday in the fairest Cape. Two weeks ago he developed severe pain on the side of his right hip; the other leg, with no back pain. Thinking it was his hip he consulted his doctor who prescribed anti inflammatory pills. But it wasn't his hip; clearly it's his back again, but a different level. Now he's vomiting profusely with a probable medication induced ulcer. It is well to remember that iatrogenic disease ("originating from the healer") causes the death of over 200,000 people annually in the USA; about a half are caused by side effects and errors of medication. Is a life without medication a pipe dream? Life without medication ezine 47. Loss of independenceElective surgery in the elderly especially must result in a period of recuperation, which may be extensive especially if affecting the lower limb.Even if the surgery is completely successful, not driving for some months may result in the patient never regaining the confidence to shop, visit friends and even doctors themselves again under their own steam. Length and quality of life is directly related to how far, and how fast we can walk. Three months of very limited walking after ankle surgery for example, may in the elderly have a catastrophic effect on their overall health, even if the operation is successful. Recently I was very against a very elderly patient having a total knee replacement; she had no knee pain and was completely independent, but her knee would give suddenly and unexpectedly. Despite a stick, falls were become more likely. Having even more troubles from lumbar stenosis, than knee arthritis, I remained unconvinced the major source of the weakness was in her knee. In a sense the knee replacement would be considered a success by the surgeon; she has no pain, and there is increased range of motion; but the knee still gives. Worse, after four months, she realised she had lost the confidence to drive, and sold her car. The loss of independence has hit her very hard. A strong and active lady has become housebound after elective surgery in the elderly; it was all unnecessary in my humble opinion since she had minimal pain prior to the operation and could walk better than she does now; and she could drive herself shopping daily. Manipulation risksThere are manipulation risks for the chiropractor that need to be weighed too.Three weeks ago a patient of nearly forty years who is turning ninety soon complained of lower back and neck pain. She has a severe scoliosis with Cobb's angle of 63 degrees; that's bad. I adjusted her back as usual but decided to treat her neck conservatively with soft tissue therapy and an activator. It didn't help her neck and she was irritated with me. She was probably right to be irritated; after all she has been a patient for a long time and I have adjusted her neck many times; and, in fact, it's the young woman on the pill who is a smoker who is really at risk. She didn't qualify on any of these counts, yet I felt on the day the manipulation risks outweighed the potential benefits. Right or wrong? Each and every case needs to be weighed on its own merits on the day. Elective surgery in the elderlyIn short, elective surgery in the elderly needs to be carefully weighed, considering all the pros and cons. Is it wise in the circumstances? Are you facing a doctor looking to make a fast buck? What are the ethics of the situation?Obviously emergency surgery is another matter altogether.
Cooling and reheating starchesThere are numerous diets that vilify carbohydrates as the cause of obesity, insulin resistance and diabetes; cooling and reheating of starches offers another insight.It is a matter confirmed by scientific research that no diets across the whole spectrum result in long term weight loss; only 5% of those who are patient enough to go on diet have one year later actually lost significant pounds, and many after put on. Usually they have gone through a lot of trouble to no good effect. In the main it's because these diets simply are not sustainable. Can you long term give up bread, potatoes, green peas, legumes, vegetables like corn and pasta? And actually is it necessary, and is it healthy, to refuse apples, sweet potatoes and winter squash, lentils and garbanzo beans simply because of their starch? These are the foods that the microbiota in the large intestine feed on, producing strongly anti inflammatory compounds, like butyrate, that are now known to help prevent autoimmune and other inflammatory diseases. Research has come up with something very interesting; simply cooling your cooked starch overnight in the fridge, and then reheating it, allows for "retrogradation" of the molecules; they reform making it difficult for enzymes in the small intestine to digest them. Instead they pass through to the colon where the bugs turn them not into glucose but into healthy short chain fatty acids like butyrate; they become what are known as resistant starches. We avoid the healthy carbs at our peril. In the desperate hope of losing weight we instead get other more serious diseases. It's the cookies and cakes, doughnuts and french fries, white rice and refined pasta, and scones and rolls that slide so deliciously down the throat that are public enemy number one, not chickpeas, butternut and apples. Find out more about resistant starch if you want permanently to lose weight without the stress of counting calories. Getting back to enjoying our food, the old fashioned way that our grandmothers in vain taught us, is the secret. She never offered you potato chips, and Sufferin' Succotash was regularly on the menu; corn and beans both banned, for example, on the Adkins and Banting diets. It was unsweetened ice tea not a cola that was on offer. In the Site Search function in the navigation bar, type 'about resistant starch' if you are interested.
Fresh from the gardenIf you read Chiropractic Help with any regularity you will know that I am passionate about healthy food and plenty of exercise; they will probably have a greater influence than any medical doctor or chiropractor on whether you will reach a healthy eighty with all your marbles and joints intact. Where possible, that means growing your own food in large measure, or having ready access to organic farm vegetables, fruit and eggs.
Firstly, a diabetic patient told me that he can eat new potatoes straight from the garden, and they produce the normal postprandial rise in sugar, but old spuds, and particularly french fries, are a disaster for his blood glucose. And secondly, our family enjoys a huge amount of unrefined carbohydrate, in the main straight from the garden, with no deleterious effect on the waistline. Thirdly, strong research confirms that whole grains, like fresh corn on the cob, have a powerful preventative effect on the epidemic of heart, stroke and diabetes that confounds the Western world; the refined flour in the modern loaf of bread of course does exactly the opposite. I am unsure of the effect of sweet corn from a can on a diabetic.
Heart stroke diabetes
There's nothing easy about getting back to slow food; it takes time and commitment, and patient energy; there simply are no shortcuts to better health and the sooner we discover the fallacy behind the fad diets, all of them, the better; some are worse than others obviously. Add to that more exercise, perhaps a lot more exercise, and you're have already taken two big steps to better health. And, yes, it does take more time. Make that time now, or you'll soon be spending even more consulting doctors of various ilks. On that note, I believe as a chiropractor that every single person should be doing some form of lower back exercises every day; I recommend you start with those done in bed before arising in the morning; whether you hurt or not; it's
called prevention. I do them myself.
Lower back exercises
BooksI don't have any new chiropractic books for you this month, but many thanks to those who continue to purchase my books, under the nom de plume, Bernard Preston; it's gratifying and helps to pay for this site.If you have never read a book by Louis de Bernieres, it's time to consider, but beware. He tackles very difficult and painful subjects, usually to do with relocation of large groups of people, war and the abuse of religion. Lest we forget, war is primarily about death and destruction, usually in the most horrific way; his descriptions are graphic. You may have heard of Captain Corelli's mandolin, but I suggest rather begin with Birds without wings. You'll laugh out aloud, but you'll cry too. Till next month, then... yours in better health.
Barrie Lewis DC and Bernard Preston DC! PS. Feel free to forward this to family and friends, your chiropractor and even your medical doctor! You can support this site by purchasing one of Bernard Preston's chiropractic books. Dirt cheap on your Kindle, tablet or smartphone.
|
| Back to Back Issues Page |